Dr. Neville Wilson
BA (Rhodes), MB.ChB, DIP.MID COG (SA), D.Obs, D Fam Med, MSc, DNH.
The current standard practice of treating patients with hypothyroidism is prescription use of levothyroxine (Eltroxin).

This practice has been adopted by many endocrinologists and family physicians ever since Eltroxin was introduced into the pharmacological market in the 1970 s, replacing the then standard of care, which was natural dessicated extracted thyroid hormone (DTE, ) which had been used by thyroid practitioners for over 100 years.
With the pharmacological push of Eltroxin, as the “only thyroid drug” on the market, use of natural dessicated thyroid hormones fell into disfavour by allopathic doctors, who followed the emerging trend of prescribing a synthetic pharmacological product in preference to a natural thyroid hormone.
In recent years the use of natural dessicated thyroid hormone extrct (DTE) has again emerged as a favourable therapeutic option for large numbers of patients who have failed to experience symptomatic relief from levothyroxine (Eltroxin).
Many of these patients have experienced favourable support by sympathetic clinicians, who have validated their support for the therapeutic use of DTE on grounds of sound scientific and clinical evidence.
Patient reports from a variety of sources suggest that large numbers of hypothyroid sufferers have experienced no clinical benefit from standard Eltroxin use, and /or negative effects of prescribed Eltroxin, with growing satisfaction from dessicated thyroid hormone support for debilitating hypothyroid symptoms.
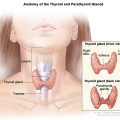
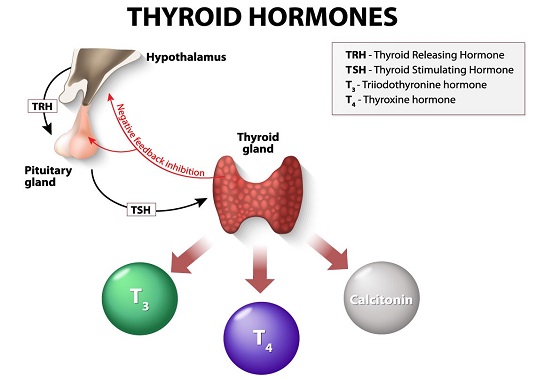
THE THYROID HORMONES T4 and T3 :
The healthy adult thyroid gland produces 2 hormones at daily levels of, 90-100 mcg levothyroxine (T4) and approximately 5-7 mcg triiodothyroinine, (T3), with an additional 25 mcg of T3 being formed daily, in the peripheral tisues through conversion of T4 to T3 by the actions of the Deiodinase enzymes, (D1 and D2) which are selenoprotein dependent.
Triiodothyonine (T3) is the metabolically active hormone, and is 10 times more potent than the storage hormone tetraiodothyronine (T4)i
While T4 ( Tetraiodothyronine) serves as a storage hormone, T3 is the metabolically active hormone, that derives in extrathyroidal tissues, liver, kidney, pituitary, skin, brown adipose tissue, skeletal muscle, CNS, and placenta, through 80-90% of the conversion from T4 to T3 via the Deiodinase Enzymes.
A third deiodinase enzyme (D3) can be expressed in most tissues, under conditions of disease or severe stress, and is also expressed during embryonic life, and may be measured by reverse T3 (rT3) evaluation.
TRANSPORT OF T4 AND T3 HORMONES:
Circulating T4 (tetraiodothyronine) and T3 (triiodothyronine) are tightly bound to thyroglobulin binding proteins (TBG), and thyroxine binding pre-albumin (TBPA) and albumin, and need to be unbound before their metabolic benefIts can be effected.
Alterations in free thyroid hormones can occur when TBG levels are increased, or decreased, as may occur under several clinical conditions, such as pregnancy, or oral contraception, or HRT, where increases in oestrogen increase the TBG binding capacity, and reduces free thyroid hormone levels.
Under these, and other clinical circumstances, therapeutic levels of active free T3 should be increased by 40-50% in order to sustain adequate tissue levels of the active hormone.
Free T3 enters target cells through specific thyroid hormone transporters, including monocarboxylate transporterS (MCT8 and MCT 10), and gains access to the cell nucleus through interaction with cell nuclear receptors (TRa and TRb), which are widely distributed throughout the body, with every cell expressing either one or both of these nuclear receptors.
When plasma T3 enters thyroid hormone target cells, it binds to the TR receptors and changes the expression of T3-responsive genes, leading to the mRNA changes that determine the positive biological effects during human development, growth, metabolism and neurocognition.
MEASURING FREE T3 LEVELS:
Many labs do not routinely measure Free T3, because of a stated “cost saving strategy”, and also because of the false perception amongst many clinicians that T3 measurements are unhelpful and therefore unnecessary. Some patients have reported their clinicians as stating that “T3 is unnecessary” and does not need to be tested.
This false perception, contradicted by critical science, has led to large sections of the population being inadequately diagnosed and inadequately treated, by ignoring possible deficiencies in Free T3 levels.
A total T4 or total plasma T3 level is a poor predictor of tissue T3 concentration, because it does not account for the intracellular production of T3 via the deiodinase pathways.
The disruption of normal thyroid hormone secretion may occur under several conditions of either nutrient deficiency (Ie iodine, vitamin D etc) or inflammatory damage to thyrocytes (THYROID FOLLICULAR CELLS) by auto- antibodies, (TPO ab & Tgab) produced by the autoimmune system, in response to toxic dietary agents, such as gliadin, contained in dietary gluten.
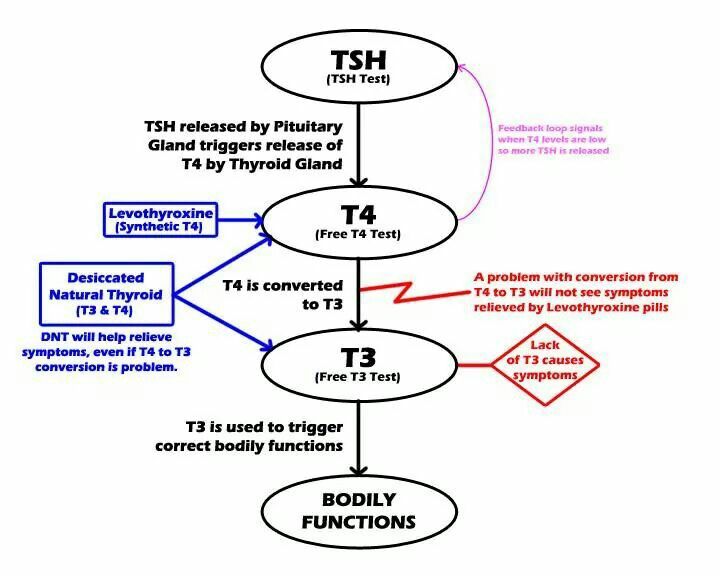
WHEN ELTROXIN (T4) IS INADEQUATE :
Patients who have the genetic and enzyme apparatus to convert their storage levothyroxine (T4) into metabolically active triiodothyronine, (T3) are able to utilise the benefits of therapeutic levothyroxine (Eltroxin).
However, In the absence of the deiodinase enzymes (tetraiodothyronine 5’ deiodinase D1 and D2) and adequate tissue levels of selenoproteins, such patients will fail to convert their storage levothyroxine, or therapeutic Eltroxin, into the active hormone triiodothyronine, also known as T3.
In these cases, standard Levothyroxine (Eltroxin) therapy for hypothyroid patients will have little or no therapeutic benefit, regardless of the dosage.
Selenium is required for the activity of the deiodinase enzymes, and is also required as an anti-oxidant in inflamed thyroid tissue as a result of Hashimoto’s thyroiditis, an autoimmune inflammatory thyroid condition, leading to eventual damage and destruction of thyroid tissue, if not appropriately managed by dietary and nutritional discretion and management.
Many patients continue to experience neurocognitive impairment despite normalization of serum TSH and T4, since T3 levels may be deficient in discrete areas of the brain, due to a variability or defect in transport enzymes or deiodinase enzymes.
This may explain the clinical benefits of T3 therapy for many patients who complain of “brain fog” and depression, and who have been wrongly diagnosed as having “chemical depression”, and inadvertently prescribed an SSRI anti-depressant drug.
Several clinical studies have demonstrated the therapeutic benefits of T3 therapy in refractory major depression. (J of Affective Disorders 115 (1-2): 230-3, Kelly TF et al, and treatment resistant biploar disorders. (J of Affective Disorders 116 (3): 222-6 (2009), Kelly TF, Lieberman DZ.)
While both T4 and T3 can cross the brain barrier, T4 can be taken up by D2 containing astrocytes and tancytes, and enter TR containing neurones to trigger its transcriptional effects. However, any defect along these pathways could affect intracellular levels of T3, and lead to localized brain hypothyroidism. Only free T3 can enter the astrocytes and tancytes and function as effective neuro transmitters.
WHEN T4 THERAPY (ELTROXIN) IS INDEQUATE :
There is a subset of patients with hypothyroidism, who do not obtain therapeutic benefit or clinical relief from levothyroxine (Eltroxin), regardless of the dosage, and may require therapeutic support from either triiodothyronine (T3) or combination therapy with T3 and T4 , as is present in dessicated thyroid extract, which contains 38mcg of T4 and 9 mcg of T3 in every grain of extract.
Natural dessicated thyroid extract is available in several products, of which the more commonly used are, NPThroid 60mg/grain, Naturethroid 65 mg/gr, or Armour, and other well known brands available internationally.
Synthetic triiodotyhronine (T3) is also available under a variety of brands worldwide, such as Thybon or Tertroxin, a 20 mcg per tablet.
Many Patients report dissatisfaction with Standard Levothyroxine therapy:
“A 2018 online survey of hypothyroid patients revealed significant dissatisfaction with standard L-T4 (Levothyroxine), with more patients having greater satisfaction with (DTE)
L-T4 / L -T3 (Levothyroxine/Liothyronine, with respect to fatigue, lack of energy, memory decline, depressed mood and weight gain. (Thyroid 2018;28:707-721, Peterson SJ)”
“Many studies reveal that increasing or changing the dosage of L-T4 (Eltroxin) does not improve symptoms of hypothyroidism. (J Clin Endorcrinol Metab 2006;91:2624-2630, Walsh JP.) and (J Clin Endocrinol Metab 2018;103:1997 208, Samuels MH)
In a 2002 study 15% of subjects treated with levothyroxine replacement therapy alone did not achieve clinical euthyroidism and experience some level of psychological improvement. (Clin Endocrinol 2002,57:577-581, Saravannan P et al)
In a large-scale cross sectional study involving about 3,900 euthyroid individuals, and about 1800 athyreotic patients kept on replacement therapy with levothyroxine, serum T3 levels were considerably lower in the hypothyroid patients, showing that levothyroxine monotherapy cannot guarantee euthyroidism in all athyreotic patients. (PloS One; 2011;6:e 22552.)
“In patients with hypothyroidism, partial substitution of triiodothyronine for thyroxine (Eltroxin) may improve mood and neuropsychological function; this finding suggests a specific effect of the triiodothyronine normally secreted by the thyroid gland “ ( N Eng J Med 1999;340:424-429,DO1:10.1056/NEJM199902113400603 )
The Conversion of T4 into T3:
“D1 and D2 are essential to catalyse he deiodination of T4 into T3 in the extrathyroidal tissues, such as brain, heart and pituitary, and with large sections of the population devoid of these enzymes because of Polymorphisms (SNP’s) at the gene level, many people continue to experience the morbid symptoms of hypothyroidism despite being medicated with Eltroxin, regardless of the dosage”.
A 2017 blind, randomized clinical study showed that the combination of polymorphims in D102 (rs225014) and MCT10 (rs17606253) enhances hypothyroid patients’ preference for L-T4 + L-T3 replacement therapy. (Eur Thyroid J 2017 July;6(3):143-151, Carle A, Faber J, et al).
60% of the patients in the study preferred the combination therepy (T3 + T4).
“The present study indicates that the combination of polymorphisms in D102 (rs225014) and MCT 10 (rs17606253) enhances hypothyroid patients’ preference for L-T4+ L-T3 replacement therapy.
In a 2009 article (J Clin Endocrinol Metab 2009,94(5):1623-1629) “Common variation in the D102 Gene predicts baseline psychological well-being and response to Combination Thyroxine Plus Triiodothyronine Therapy in Hypothyroid Patients”.
A 2009 European Journal of Endocrinology article reports the outcome of ‘Effect of combination therapy with thyroxine (T4) and 3,5,3’-triiodothyroxine versus T4 monotherapy in patients with hypothyroidism, a double-blind, randomised cross-over study”, and concludes , “ combination therapy in groups treated with T3 20mcg once daily was superior to monotherapy by evaluating several QOL, depression and anxiety rating scales as well as patients own preference. (Eur J Endocrinol Dec1 2009, 161,895-902)
It is clear from my long-standing treatment of Hypothyroidism, spanning more than 30 years, that common symptoms of an underactive thyroid gland, may include, high levels of unexplained fatigue, brain fog, depression, muscle pain, hair loss, and unwanted weight gain, despite improvements in dietary habit, or increased physical activity and exercise programmes.
Furthermore, there is evidence that many cases of infertility result from undiagnosed and untreated hypothyroidism, as well as unexplained miscarriages, and intra-uterine fetal deaths.
In these cases, many patients report that long standing symptoms, as above, do not abate, regardless of therapeutic levels of Eltroxin (T4), where levels of free T3 have not been evaluated, or adequately supported.
Reliance on TSH and T4 alone for Thyroid gland function is unreliable as a diagnostic or therapeutic guide.
“Furthermore, the reliance on the standard reference range for TSH at (0.4-5.0mUI) is likely to underestimate and result in under treatment of hypothyroidism, since tissues are closest to euthyroidism at TSH 0.3-3.0 mU/L (J Clinic invertig2015;125:769-781, Werneck de Castro)”
Thyroid status and dose adequacy of T4 (Eltroxin) cannot adequately be defined by the putative gold standard of TSH in these conditions because TSH concentrates within the accepted range may not invariably signal optimum concentrates of the peripherally active free T3. (Euro J Endocrinol 2013;168:271-280, Hoermann R.)
“These facts challenge the perceived role of TSH as an exclusive standard in assessing dose adequacy in thyroid replacement therapy”.
“Safety concerns about the use of T3 or T4/T3 replacement therapy in hypothyroidism are unfounded, as revealed in the Scottish TEARS study in 2016, with no increase in risk for cardiovascular disease, atrial fibrillation or fractures, when adjusting for age. (Clin Endorcrinol 2016;85:918-925, Leese GP etal)”
Because of the growing awareness of clinical benefit for combined T4/T3 treatment for hypothyroid patients, demands for combination therapy have increased significantly in USA, Canada, Australia and most European countries in recent years.
(Thryoid 2019;29:44-52, Jonklass J etal)
(Eur Thyroid J 2015;4:174-180, Michaelson LF et al)
Since various combinations of L-T4/ L-T3 are available to physicians treating patients with Hypothyroiism, evaluation of the most effective therapeutic option is best effected through co-operation between therapist and patient in a treatment trial, giving cosideration to symptom relief and quality of life as eported by the patient.
-Dr Neville S. Wilson.
BA (Rhodes), MB,ChB (UCT), D.Obs (UCT), DIP MID (COG) SA., D Fam Med, (Pret), MSc, DNH.
Diplomate of the College of Obstetricians & Gynaecologists of SA.