
VITAMIN K2 AND OSTEOPOROSIS
A Non- Pharmacological Approach to the Management of Osteoporosis
by Dr. Neville Wilson
November, 2014.
Osteoporosis is a serious and potentially debilitating condition, in which human bone fragility can give rise to unsuspecting fractures in vulnerable elderly males and females, with increased risk for morbidity and mortality.
The common perception that osteoporosis affects only females is false, and may limit the detection and diagnosis of bone disease in males, allowing the condition to advance without appropriate intervention or treatment.
Some researchers predict that 1 out of every 4 males will sustain an osteoporotic fracture in their lifetime. (1)
BONE STRENGTH :
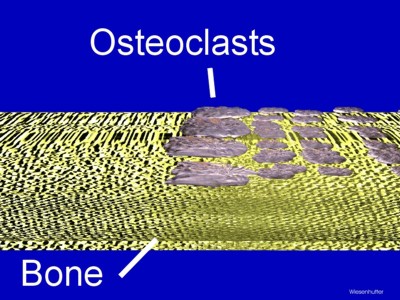
Skeletal bones are living tissue and in a constant state of renewal, with old bone cells being dissolved by osteoclasts, and new bone cells being laid down by osteoblasts.
The synergistic activity of osteoclasts and osteoblasts enables remodeling of bone tissue and structural integrity for the entire skeletal system.
While it is well established that calcium and vitamin D, in it’s active form, are prerequisites for new bone formation, public and professional awareness is scant regarding the important role that vitamin K2 has in protecting bones against brittle decay.
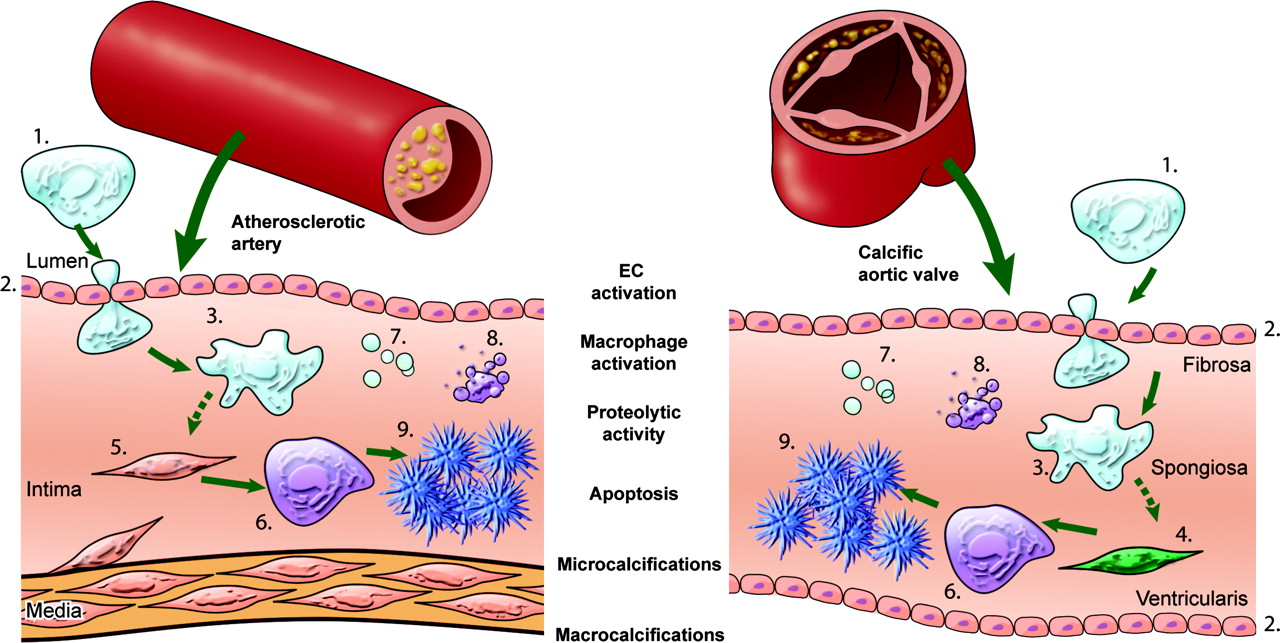
Emerging scientific evidence is strong, not only for the protective role of vitamin K2 in bone health, but also for its capacity to reverse arterial calcification and provide protection against atherosclerosis, a risk for cardiovascular disease.
BONE REMODELLING:
Vitamin K2 is essential for regulating calcium balance in the body and improving bone mineral density.
Osteoblasts remodel the cavities created by osteoclasts, by laying down calcium in response to osteocalcin and vitamin K2 activity.
Osteocalcin (OC) is one of 3 identified carboxy glutamate (Gla) proteins, secreted by the bone building osteoblasts, which draws calcium from the blood and layers it in the cavities created by the osteoclasts. ( A deficiency of vitamin K2 causes under carboxylation of osteocalcin and diminished capacity for laying down calcium in bone matrix). (2)
Vitamin K2 secures bone integrity by turning off excess osteoclast activity, and by supporting the action of osteocalcin by drawing calcium from the blood and importing it into bone tissue.
Recent studies have identified the protective role of Vitamin K2 in bone and cardiac health, and how a deficiency of vitamin K2 can give rise to brittle bones, as well as to premature hardening of the arteries. (2) (3) (4) (5)
DRUG THERAPY IN OSTEOPOROSIS :
Pharmaceutical agents, widely prescribed by doctors for protection against osteoporosis have been shown to have limited success in maintaining prolonged bone health or conferring mortality benefits.
Evidence suggests that their benefits do not extend beyond 3 or 4 years beyond which time their risks for adverse events may increase.
The potential for serious adverse effects from several widely used anti-osteoporosis agents have been widely documented, with reports of osteonecrosis of jaw bone and atrial fibrillation ( a potential risk for stroke) being caused by prolonged use with bisphosphonates. (6) (7).
While certain drugs can temporarily increase bone density, they generally fail to support the natural cycle of regeneration and resorption that is essential for bone strength. (8)
As a precautionary measure, the critical re-assessment of bone density and bisphosphonate treatment by clinicians has been advised by some experts. (9)
Risks for Developing Osteoporosis :
Bone is a composition of matrix protein, calcium compounds, and several trace minerals which include magnesium, silicon, boron and zinc.
Many factors are involved in the excessive resorption of bone mass, causing demineralization and bone fragility.
These may include sub-optimal nutrition, excess alcohol intake, age related hormone decline, and lack of weight bearing exercises.
In addition, insulin resistance, elevated blood sugar and advanced glycation (Interaction between blood sugar and proteins) can advance demineralization of healthy bone.
Studies with Vitamin K2 ( Menaquinone 4) :
In a 1996 population based study involving 113 post menopausal females, reduced vitamin K2 status was associated with abdominal aortic calcification and also reduced bone mineralization. The benefit of vitamin K2 was shown for both vascular and bone health. (4)
More recent studies have demonstrated the several actions of Vitamin K2 as a protector of bone health (3) (2), and a meta-analysis by Cockayne et al in 2006 documented the protective benefit of vitamin K2 in maintaining bone mineralization. (9)
In the 2004 Rotterdam Heart Study dietary intake of vitamin K2 (menaquinone) was associated with a reduced risk of coronary heart disease through calcium withdrawal from the circulation. (10)
Vitamin K2 and Warfarin ?
Patients who use anticoagulant drugs (like Warfarin) may be routinely advised to avoid food containing vitamin K, since in theory, Vitamin K may interfere with the anti-coagulant properties of vitamin K.
The unfortunate effects of this advice is to create a vitamin K2 deficit, with an added risk of developing valvular and arterial calcification, as well as poor bone mineralization.
It is recommended that patients and clinicians work closely together to moniter INR levels so that a balance between blood thinning and blood clotting is maintained, without compromising the nutritional requirements for vitamin K2 for bone health, and the avoidance of arterial calcification.
In a 1999 Japanese study a high dose of Vitamin K2 given concomitantly with Warfarin reduced the effect of Warfarin on thrombosis, but did not enhance the occurrence of thrombosis more than without warfarin treatment. (11)
CONCLUSION :
Since Vitamin K was discovered in 1929, a plethora of studies have demonstrated it’s several health benefits, other than only for healthy blood clotting (Vit K1).
The past decade has witnessed a large body of research outcome focusing on Vitamin K2 metabolism, and it’s benefits for bone health and vascular health, in addition to suppression of chronic inflammatory factors.
Several studies have shown the multiple benefits of vitamin K2, apart from improving bone mineral density. Vitamin K2 has been shown to reverse arterial calcification (12), reduce prostate cancer risk (13), and support anti-cancer mechanisms by inhibiting the pro-inflammatory factor nuclear factor kappa B (NF-kB) (14)
At risk candidates for developing osteopenia, osteoporosis, cardiac disease or diabetes, would improve their protective status by including Vitamin K2 rich foods in their diets, such as grass fed organic animal products, such as butter, egg yolk, fermented cheeses like Brie or Gouda, and fermented foods such as natto or fermented vegetables.
Dr. Neville Wilson.
November 2014.
REFERENCES:
Euro J Epid 2009; 24(8):441-8 Ahmed, L A.
Vit Horm 2008; 78:393-416, Bugal S.
Nutrition 2006 July; 22(7-8): 845-52
Calcif Tissue Int 1996 Nov; 59(3):352-6
Kardiol 2001; 90 (Supp): 357-63
BMJ 2010; 341:c444, Green L E.
Am J Cardiovasc Drugs, 2010; 10(6):359-67 Howard, P A.
Calcif Tissue Int 2010 June; 86(6): 421-35
Circ Intern Med 2006 June, 26: 166(12): 1256-6
J Nutr, 2004, Nov; 134(11):3100-5 Geleijnse, J M
Nihon Yakurigaku Zasshi 1999 Mar; 11(3): 185-92
Blood 2007 April 1; 109 (7): 2823-31
Am J Clin Nutr 2008 April; 87 (4): 985-92
Chem Cancer Res 2007, April 1; 13(7): 2236-45
Nutrition 2001 April; 17(4):3415-21
Int J Epid 2000 Oct; 29(5):832-6
00O00

I take coumadin for a mechanical heart valve and atrial fibrillation. I have osteoporosis in my hip and osteopina eslsewhere. My arms are normal. Thank am scared to take vitamin k2 . How often would I have to get my Inc to be safe.
Thank you
Sheena